


🧪 Designing Clinical Trials with QOL Endpoints in NSCLC:
More Than Just Survival


🧬 Why This Matters: A Personal Note
One disease I’ve worked a great deal in is non-small cell lung cancer (NSCLC). I consider myself lucky to have been one of the first researchers involved in the pivotal study that led to the registration of crizotinib in ALK-positive NSCLC back in 2011.
That was a clinical milestone. But if I’m honest, most of the trials I’ve worked on didn’t have that kind of impact. Still, in each of them, we did our best to understand how treatments affect not just survival, but quality of life—whether through radiotherapy protocols, maintenance strategies, or large-scale reviews looking across dozens of trials and even in health utilities.
Over the years, we published two major reviews on QOL in NSCLC trials. The conclusion?
Most randomized controlled trials in NSCLC were historically methodologically weak when it came to QOL.
We often saw poor data collection, inadequate tools, and a lack of integration into clinical decision-making.
I hope—and believe—that things are improving. But designing trials that take QOL seriously is still far from easy.
And that’s why I wrote this post. Its not going to answer all the questions, but it will at least show some of the challanges we all face when desiging QOL trials in the NSCLC space.
🌬 Why QOL Matters in NSCLC
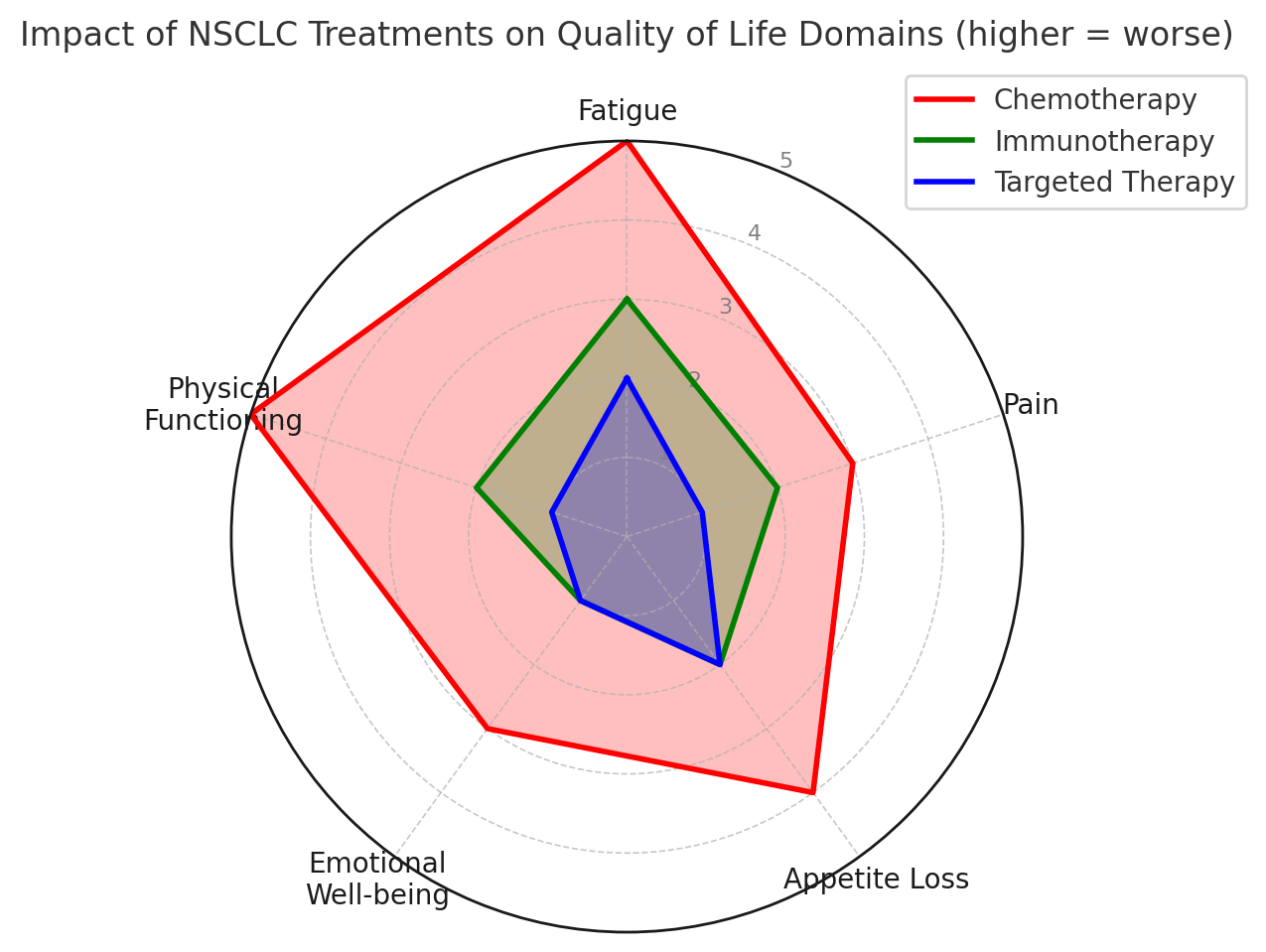
NSCLC remains one of the most diagnosed cancers globally. And despite therapeutic advances—including immunotherapy, targeted agents, and combination regimens—symptom burden remains high. Fatigue, breathlessness, pain, and cough are daily realities for patients.
Crucially:
Many therapies (especially in the second-line or later settings) extend survival by just a few months or even weeks in some cases.
Patients and clinicians increasingly prioritize function, independence, and symptom relief just as much as longevity.
So measuring QOL isn’t a soft science—it’s central to understanding clinical benefit.
🧠 Step-by-Step: How We Integrate QOL into NSCLC Trials
📖 For reference, the FDA’s Patient-Focused Drug Development (PFDD) guidance (especially the series released between 2019–2022) outlines best practices for integrating PRO measures, emphasizing the importance of tools that directly reflect patients' lived experience and advocating for early engagement with regulators. You can find the most recent guidance on the FDA website.
1. Choose the Right Tool for the Population
EORTC QLQ-C30 + QLQ-LC13 (lung-specific module) are often considered gold standards in Europe. Some five years ago LC 13 has recently been updated, to the EORTC LC29. Which one do you use? I suggest it depends on the treatment and study design.
FACT-L is widely used in U.S. trials. The MDASI lung is a very good tool ,focused on symptoms.
Consider completion burden—can your patients handle a 30+ item questionnaire every cycle?
📝 Tip: Avoid overloading. Use only what supports your hypothesis and meets regulatory needs.
We also just submitted a new review paper comparing the EORTC lung module and the FACT-L, which we hope will serve as a practical guide to help researchers decide which tool best fits their trial design and population. Come back to me if you are interested in this paper…
2. Define a Meaningful Change
For QLQ-C30, a 10-point change is often considered clinically important. But this is really a historical view..
Align with FDA guidance on Minimal Important Difference (MID) using anchor-based or distribution-based approaches.
📌 However, the field of MID is very complex, and 10 points is only a "rule of thumb." I've written 10–15 papers on the topic of clinical significance, and I’d say: if you're interested, reach out to me. We can discuss it—because different regulators have different interpretations, and HTA bodies use different thresholds for what counts as a clinically meaningful change!
📌 “Statistically significant” ≠ “Clinically meaningful”
3. Timing Is Everything
Capture QOL at time points that are clinically meaningful. Let your hypothesis drive this. It’s not uncommon for timings to follow the pattern below, but there is no standard. You need to adapt your timing to the treatment, disease stage, and patient population:
Baseline
Post-cycle 2
End of treatment
First disease progression
Follow-up (e.g., 90 days post)
Missing data tends to come from the sickest patients—the very people whose experiences matter most. Again, how to address this is very complex, and I’ve written a few papers that explore these issues. If you’d like to dive deeper, I’d be happy to discuss or share references.
4. Integrate QOL with Clinical Endpoints
Aim to link:
Tumor response → symptom improvement
Toxicity → impact on daily functioning
Time to deterioration (TTD) → early signs of QOL decline
HTA bodies and regulators may now be looking for net clinical benefit—the blend of survival and tolerability. This is where some think that QOL data shines. However, it can also be an area of intense debate. Personally, I don’t always support mixing QOL with clinical endpoints, as it introduces many complexities and interpretive risks. I am also not a big fan of TTD, for many reasons, and even some regulators explain the need to take care when using this approach.
📊 Trial Example: Phase III in 2L NSCLC
Let’s say:
Drug A (chemo + novel immunotherapy) vs docetaxel
Primary endpoint: PFS
Key secondaries: OS and global QOL (using QLQ-C30 & LC13)
You might include:
QOL assessment at baseline, each cycle, end of treatment, and day 90 follow-up
A ≥10-point drop in dyspnea as your TTD event (or better still look for the more recent paper we published in MID for NSCLC). Plus check your scales, and check the direction you expect to see the change, as all can influence the MID levels.
A subgroup analysis in patients >70 focused on tolerability
This trial doesn’t just show how long patients live—it shows how well they live.
🚧 Barriers and Real-World Challenges
Let’s be honest—QOL data collection is often a logistical mess:
Sites forget or de-prioritize PRO forms
Data is incomplete or delayed
Digital tools can be underused or poorly configured
Patients can be overwhelmed with paperwork
But we don’t give up. We design smarter. We advocate harder.
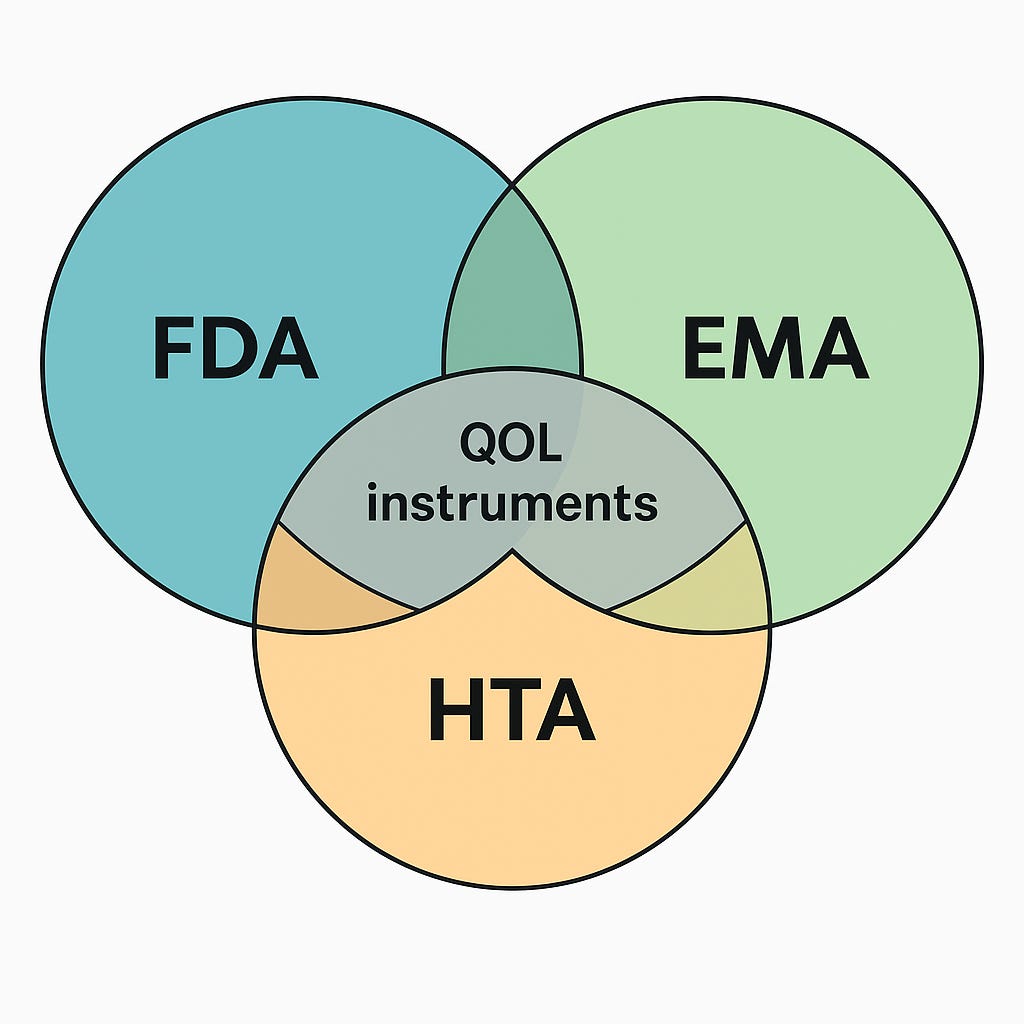
🤝 How to Please All Stakeholders: Regulators, HTAs, and Patients
One of the hardest parts of building a QOL strategy in NSCLC isn’t the science—it’s the regulatory politics.
The Problem:
FDA prefers tools like PROMIS or perhaps more symtom based tools such as the PRO-CTCAE.
EMA leans toward EORTC QLQ-C30/LC13.
HTA bodies (e.g. NICE, IQWiG) want EQ-5D for health economics.
But we can’t ask patients to fill out 4+ overlapping surveys every visit.
🧩 Practical Solutions
✅ 1. Core measure + Satellite Model
Use a core instrument (eg. QLQ-C30 or FACT-L)
Add a short utility tool (like EQ-5D) for HTA purposes
Include symptom subscales tied to your treatment’s expected benefit (e.g., fatigue, cough)
🌍 2. Align Early
Seek Scientific Advice from EMA and Type C meetings with FDA
Use parallel EMA/HTA consultations (via EUnetHTA) to align tools
🔄 3. Build PROs into Label and Access Planning
Plan to show:
Time to deterioration (if you like this endpoint.. !)
Proportion of patients improving
Anchor-based clinical links (e.g., cough relief vs response rate)
These insights feed label claims, payer dossiers, and real-world value arguments.
📱 4. Go Digital, But Thoughtfully
Use smart skip logic
Enable remote completion
Collect feedback from patients during the trial
🤔 5. Be Transparent in Protocol Design
Justify tool selection in your protocol - very well… and your scales if QOL is going to be within your statistical planning.
Include fallback analysis plans (e.g., mapping QLQ-C30 to EQ-5D utilities)
QOL isn’t the cherry on top—it’s the flavor of the whole cake.
If your therapy adds time, you must show what kind of time it is.
If your strategy burdens patients, they’ll show it in attrition and noncompliance.
Design carefully. Ideally use experts, who have spent years doing this work! Justify clearly. Respect what matters most to patients.
👋 Final Thought
QOL in NSCLC isn’t about sentimentality—it’s about science, survival, and what makes survival worth it.